Ultrasound-guided peripheral i.v. cannulation is one of the most used ultrasound-guided procedures. It is often the first-time clinicians experience the benefits of PoCUS, particularly PoCUS guided procedures.
How do you go about learning? Being a hands-on skill, there is no substitute for practical training. However, the resources below will give you the theoretical knowledge.
The boring bits
People often skip this step but it’s worth getting up to speed at the start of your PoCUS journey.
Learning the basics of ultrasound physics makes interpreting images easier, especially when something doesn’t look right. It’s particularly important to understand why you might have a limited view of the needle , or possibly not be able to see it at all. The physics resources can be found here:
You need to know how to operate the machine you will use. At a minimum you will need to be able to select the correct transducer, orientate it correctly, change the depth and alter the gain the get the best possible image. Have a look at our resources on machine controls or use the manufacturer pages to find the instructions for the machine you’re using:
Aseptic technique
Follow your local policy with regards to sterile coverings for the transducer and the use of sterile ultrasound gel.
Ultrasound guided peripheral i.v. access can be achieved using an in-plane or out-of-plane technique. You may hear the in-plane technique referred to as the ‘long-axis’ approach.
The out-of-plane technique describe san approach with the needle perpendicular to the ultrasound beam. This is referred to as the ‘short-axis’ approach. The beam is moved as the needle tip is advanced so other terms are used to describe this technique including, ‘chasing the tip’ or ‘walking the tip’.
PoCUS 101 gives a great explanation of both the in-plane and out-of-plane methods and covers all the other parts of this procedure.
The two part series by PoCUSGeek provides a good overview of both in plain and out of plane technique and highlight the risks in relying on Doppler when determining which vessel to target. It suggests how to confirm correct placement of the cannula.
These resources are shown below.
All of the peripheral iv access resources are linked at the bottom of this page.
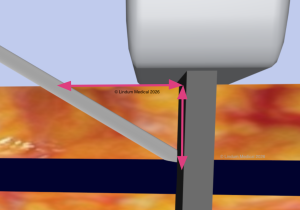
If the vessel is 10mm deep and you use an approach angle of 45°, you will use 14 mm of cannula length to reach the vessel. Decreasing the angle to 30° will give a better image but now needs 20mm of cannula to reach the same vessel. Target a vessel at 20mm deep with the same approach angle and you’ll need 40mm of cannula to reach the vessel. A lot of standard cannulas will be shorter than this, so it is easy to see why they might fail. During insertion you may also be compressing the subcutaneous tissue with the probe making the vessel appear less deep than it actually is.
Longer cannulas exist for this purpose, such as the Introcan Safety® Deep Access by BBraun. The 18G version has a length of 64mm.







 cannulation")






